
Does Growth Hormone Affect Dementia Risk?
How to Support Growth Hormone After Midlife Without Taking Hormones

Growth hormone usually enters the longevity conversation through body composition.
That makes sense.
Growth hormone affects muscle, bone, fat metabolism, and tissue repair. But growth hormone also sits inside a larger overnight process that includes sleep depth, brain health and dementia.
In a UK Biobank analysis of 369,711 adults, IGF-1 - the hormone the liver produces in response to growth hormone - tracked hippocampal volume.
Specifically, lower IGF-1 was associated with
a smaller hippocampus,
less white matter volume, and
more white matter lesions.
The study adjusted for sex, age, ethnicity, educational attainment, smoking status, alcohol intake frequency, vegetable and fruit intake, body mass index, hypertension, diabetes, total cholesterol, and C-reactive protein.

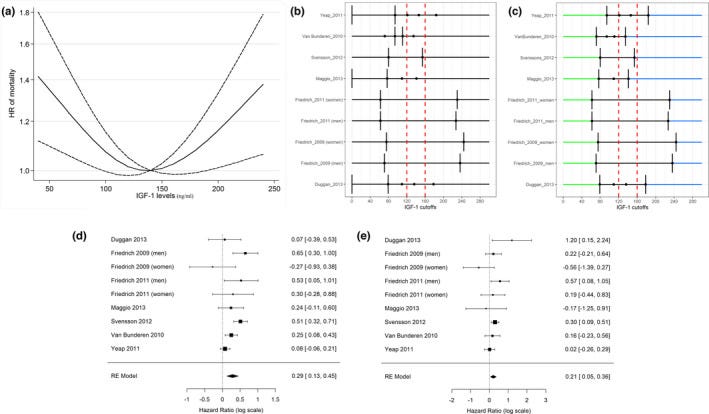
In a separate long-term study, adults in the lowest IGF-1 quartile had a 51% higher risk of developing Alzheimer's dementia over 7.4 years.
Growth hormone is also tied to the part of sleep that matters for overnight restoration. The largest growth hormone release of the 24-hour cycle usually occurs during the first 60-90 minutes of sleep, when slow-wave sleep is deepest.
During slow-wave sleep, cerebrospinal fluid movement through the glymphatic pathway increases. Recent human data show that sleep-active clearance helps move amyloid beta and tau (proteins involved in Alzheimer's disease pathology) from brain tissue.
But is more growth hormone better?
In this article we'll discuss:
what the longevity data supports in relation to growth hormone
which factors support healthy growth hormone function
which factors disrupt growth hormone release or reduce IGF-1 ( insulin-like growth factor-1) response
9 things you can do today, to improve growth homone function for optimal brain health & longevity without using peptides or exogenous hormones, regardless of your age
Let's get started.
Section 2. The IGF1 (insulin-like growth factor-1) paradox - why longevity data does not support maximizing growth hormone
The assumption behind peptide use is that restoring youthful growth hormone output is desirable.
The longevity data is more nuanced.
Insulin-like growth factor-1 is the primary liver-produced hormone that responds to growth hormone. It carries many of the tissue-level effects associated with growth hormone: muscle protein synthesis, bone density maintenance, and cellular repair.
Large pooled analyses suggest that insulin-like growth factor-1 has a U-shaped association with all-cause mortality.
At the low end, lower insulin-like growth factor-1 is linked with frailty, sarcopenia, cognitive decline, and bone vulnerability.
At the high end, higher insulin-like growth factor-1 is linked with proliferative concerns, with acromegaly as the human example of chronic growth hormone and insulin-like growth factor-1 excess.
The longevity target is the middle of the range.
There is also a timing question.
Growth hormone is normally released in pulses, with the largest release tied to early slow-wave sleep.
A single lab value does not show whether growth hormone was released at the expected time, whether insulin-like growth factor-1 stayed in a physiologic range, or whether the tissue response was optimal.
So what affects whether the nightly growth hormone release happens at the right time?
Section 3. Factors that support healthy growth hormone function
1. Sleep depth and continuity
The largest growth hormone release of the day usually occurs during the first episode of slow-wave sleep. In one study of healthy men aged 16-83, slow-wave sleep fell from 18.9% of total sleep time in young adulthood to 3.4% by midlife, while growth hormone release fell in parallel.
What matters is more than total sleep duration. The depth and continuity of the first sleep block determine whether the early sleep-linked growth hormone release has a place to occur.
Sleep fragmentation can reduce the early growth hormone release even when total sleep time looks adequate. Chronic sleep restriction can also move growth hormone release into smaller events later in the sleep period.
Across midlife, the growth hormone change tracks the loss of slow-wave sleep closely.
By the way, if sleep after 40 no longer responds to the usual strategies, I’m opening private early access to my science-backed sleep intelligence app built exclusively for men 40+, coming to iOS and Android.
It is tailored to men’s sleep physiology after 40, including testosterone, growth hormone, and GABA-related changes
Join the waitlist - or share this with someone you care about who could benefit:
2. Circadian alignment
In the early sleep period, growth hormone-releasing hormone activity is more supportive of release, while somatostatin restraint tends to be lower.
Both circadian timing and sleep onset contribute to growth hormone release. The circadian component means a late or biologically mismatched sleep period can change the size and timing of the release.
Adequate sleep at a mismatched time can still contain slow-wave sleep, but the hormonal context around that sleep is different.
When sleep onset moves across a wide range, the circadian clock has a harder time aligning sleep pressure, melatonin timing, and the growth hormone-releasing hormone/somatostatin balance.
3. Insulin
Growth hormone release is lower when fasting insulin and abdominal visceral fat are higher.
When insulin drops between meals, the pituitary is less exposed to one of the metabolic conditions associated with lower growth hormone release. When insulin stays elevated through frequent eating, late-night intake, or caloric excess, the first deep sleep block begins under a different endocrine state.
Free fatty acids also matter. Abdominal visceral fat can raise free fatty acid delivery to the liver and pituitary, which can further reduce growth hormone release.
4. Testosterone and estrogen
Testosterone and estrogen help shape growth hormone pulse size and the downstream insulin-like growth factor-1 response.
In men, testosterone can support growth hormone release directly. But the insulin-like growth factor-1 response also depends partly on aromatization to estradiol. When aromatization is blocked, testosterone can still affect growth hormone release, while the insulin-like growth factor-1 response may be smaller.
In women, estrogen can support growth hormone release by reducing somatostatin tone at the hypothalamus.
In midlife, testosterone function becomes more easily disrupted in men, and estrogen changes through perimenopause and menopause in women.
Section 4. The factors that disrupt healthy growth hormone function
1. Somatostatin affects growth hormone release and timing
Somatostatin is the hypothalamic hormone that suppresses growth hormone release.
It has appeared throughout this article because sleep timing, insulin exposure, cortisol physiology, inflammation, alcohol, and energy state all interact with the balance between growth hormone-releasing hormone and somatostatin.
The human data are more nuanced than the old shorthand. Growth hormone-releasing hormone stimulates release. Somatostatin reduces the size of that release. Ghrelin and related ligands can amplify the pituitary response.
Aging tends to involve
lower growth hormone-releasing hormone activity,
altered ghrelin rhythm, and
higher somatostatin restraint.
That combination can reduce growth hormone pulse size even when the pituitary can still respond.