
Can Histamine Intolerance Cause Sleep Problems?
Histamine is one of the brain's wake-promoting neurotransmitters. Reduced histamine clearance can make sleep more fragmented after sleep onset.

Yes - and histamine intolerance can contribute to sleep problems, especially sleep maintenance insomnia. Histamine intolerance occurs when the body cannot break down histamine efficiently, usually due to low diamine oxidase (DAO) enzyme activity. In a prospective prevalence study of 167 adults with insomnia-related symptoms, 82.6% carried AOC1 variants associated with DAO deficiency. Histamine is a wake-promoting neurotransmitter in the brain's tuberomammillary nucleus, and mast cell mediators may add another arousal pathway when histamine-related inflammation is active.
When the body cannot break down histamine efficiently, histamine-related arousal pathways may stay more active during the sleep period - and standard sleep supplements that interact with mast cell pathways may be insufficient when histamine load or mast cell activation is part of the sleep problem. Addressing histamine clearance may improve sleep quality, daytime energy, and cognitive function over time when histamine burden is one of the active contributors. This article covers how diamine oxidase enzyme deficiency connects to insomnia, why common sleep remedies may be incomplete when histamine is elevated, what the research shows about histamine-targeted approaches, and how mast cell activation extends that disruption.
What Is Histamine Intolerance and How Does It Affect Sleep
Histamine intolerance is not an allergy - it is a reduced capacity to break down histamine, typically from low diamine oxidase (DAO) enzyme activity. When histamine accumulates faster than the body can break it down, histamine-related arousal pathways may remain active during the sleep period. In a prospective prevalence study of 167 adults with insomnia-related symptoms, 82.6% carried genetic variants associated with DAO deficiency, and 88% reported difficulty staying asleep as their primary complaint (Lopez Garcia et al., 2024).
Histamine is one of the brain's primary wake-promoting neurotransmitters. Histaminergic neurons in the tuberomammillary nucleus (TMN) - a small cluster in the posterior hypothalamus - fire during wakefulness and stop firing during sleep (Thakkar, 2011). When histamine-related signaling remains elevated, that wakefulness drive may make sleep more fragmented.
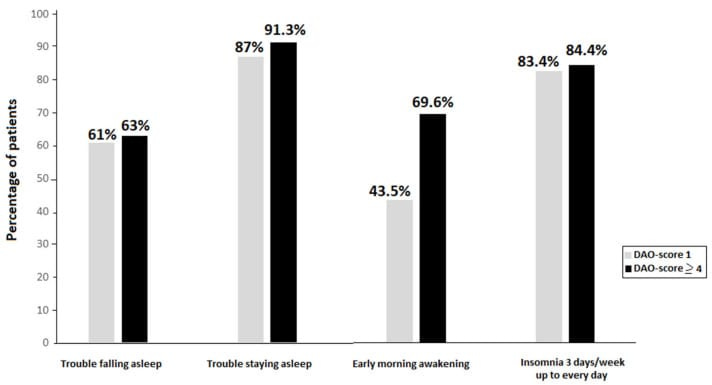
The enzyme responsible for breaking down histamine in the gut and bloodstream is diamine oxidase (DAO). Genetic variants in the AOC1 gene - the gene encoding DAO - reduce the body's capacity to degrade histamine from food and from endogenous mast cell release. In a 2024 prospective prevalence study of 167 adults presenting with insomnia-related symptoms, 82.6% carried AOC1 variants associated with DAO deficiency. Among those with higher genetic burden (four or more single nucleotide polymorphisms), rates of sleep maintenance problems and early morning awakening were elevated compared to those with fewer variants (Lopez Garcia et al., 2024).
The insomnia pattern in histamine intolerance tends to look different from stress-related or circadian-related sleep problems. The predominant complaint in Lopez Garcia's cohort was difficulty staying asleep (88%), followed by difficulty falling asleep (60.5%). That maintenance-dominant pattern - falling asleep at a reasonable time but waking repeatedly or too early - is consistent with histamine-related arousal contributing to wakefulness during the second half of the night.
Beyond sleep, histamine intolerance produces a constellation of overlapping presentations. In a study of 77 individuals with histamine intolerance, Tamasi and Kalabay (2025) documented respiratory issues in 95%, bloating in 94%, headache in 91%, fatigue in 83%, and postprandial drowsiness in 81%. The drowsiness-fatigue combination is often misattributed to poor sleep alone, when histamine excess may be contributing to both daytime fatigue and nighttime waking.
One reason histamine intolerance goes unrecognized for so long: the presentations vary from episode to episode in the same person after similar exposures, making it difficult to identify a pattern.
What Is the Diamine Oxidase Enzyme and How Does It Affect Sleep
Diamine oxidase (DAO) is the primary enzyme responsible for breaking down histamine in the gut and bloodstream. When DAO activity is low - from genetic variants, gut inflammation, or certain medications - histamine from food and mast cell release accumulates instead of being cleared. A 2026 randomized controlled trial found that DAO supplementation improved sleep quality measures, and participants using melatonin had greater insomnia severity improvement with DAO than with placebo (Ferrer-Garcia et al., 2026).
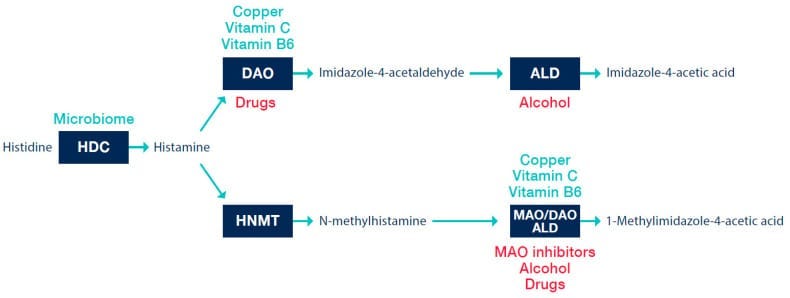
DAO is produced in the intestinal mucosa. Its primary job is to degrade histamine before it enters the bloodstream. When DAO activity is sufficient, dietary histamine - from aged cheeses, fermented foods, cured meats, alcohol - gets broken down in the gut. When DAO activity is low, that histamine passes into circulation and adds to whatever histamine the body is already producing through mast cell activity.
Several factors reduce DAO activity beyond genetics. Gut inflammation can damage the intestinal cells that produce DAO. Alcohol inhibits DAO directly. Certain medications - including some NSAIDs and antiarrhythmics - also reduce DAO function (Hrubisko et al., 2021).
When a genetic predisposition toward low DAO combines with any of these factors, nighttime histamine burden may remain elevated during the hours when wakefulness-promoting histamine signaling should be lower.
The connection between DAO support and sleep improvement has recent evidence. In a 2026 randomized, double-blind, placebo-controlled trial, 101 adults with insomnia and confirmed AOC1 gene variants received either DAO supplementation or placebo for 28 days. The DAO group showed improvements in Pittsburgh Sleep Quality Index scores - including sleep efficiency and reduced sleep medication use - compared to placebo. Among participants who were also taking melatonin, insomnia severity improvements were greater in the DAO group at both day 7 and day 28 (Ferrer-Garcia et al., 2026).
The DAO-plus-melatonin finding matters. For people whose insomnia involves histamine accumulation, melatonin alone may be insufficient because it does not address the histamine excess. Adding DAO enzyme support may reduce one wake-promoting input while melatonin supports circadian-driven sleep onset. Without addressing the histamine burden first, melatonin is working against a wakefulness drive it was not designed to override.
The mechanistic link is biologically plausible but should be stated carefully: histamine promotes wakefulness through H1 receptor activation in the TMN, while DAO primarily reduces peripheral histamine burden. Histaminergic neurons fire exclusively during wakefulness and cease firing during NREM and REM sleep (Thakkar, 2011). Reducing circulating histamine - whether through DAO supplementation, dietary histamine reduction, or both - may reduce one contributor to nighttime arousal in people whose sleep disruption is histamine-related.
Can Mast Cell Activation Syndrome Cause Insomnia
Yes. In a study comparing 553 individuals with MCAS to 558 controls, those with MCAS had elevated rates of severe chronic insomnia across both sexes. MCAS involves pathological mast cell degranulation that releases not only histamine but serotonin, cytokines, and prostaglandins - creating compounding sleep disruption that extends beyond what antihistamines alone can address (Weinstock et al., 2025).
Mast cell activation syndrome (MCAS) is a condition in which mast cells degranulate inappropriately - releasing inflammatory mediators without a true allergic trigger. Where histamine intolerance involves impaired breakdown of histamine, MCAS involves excessive production and release of histamine alongside many other mediators.
MCAS carries a heavy sleep burden. Weinstock et al. (2025) surveyed 553 individuals with MCAS and 558 controls and found that insomnia was among the neuropsychiatric conditions elevated in MCAS across both sexes. Women with MCAS reported higher rates in 18 of 19 neurologic categories and all 14 psychiatric categories; men reported higher rates in 17 of 19 neurologic categories and 8 of 14 psychiatric categories. When those with MCAS rated the effectiveness of various approaches for their neuropsychiatric presentations, antihistamines received a rating of 6.3 out of 10 - outperforming benzodiazepines at 5.6 out of 10. That finding is relevant, but it should be read as patient-reported neuropsychiatric relief overall rather than an insomnia-specific drug comparison.
MCAS also creates sleep disruption through pathways beyond histamine alone. Weinstock et al. (2020) found that 40.8% of individuals with MCAS had restless legs syndrome, compared to 12.9% of spouse controls. In women with MCAS, there was an odds ratio of 6.7 compared with the general U.S. female population. Restless legs syndrome disrupts sleep onset and sleep maintenance independently - meaning people with MCAS can face both histamine-driven early awakening and movement-related sleep fragmentation at the same time.
The compounding nature of MCAS is what distinguishes it from isolated histamine intolerance. When mast cells degranulate, they release histamine, but also prostaglandins, serotonin, cytokines (including TNF-alpha and IL-6), and tryptase. These mediators can influence arousal, pain, inflammation, autonomic tone, and movement-related sleep disruption through different pathways. This is why people with MCAS often describe their insomnia as resistant to every approach they have tried: each remedy addresses one pathway while several others remain active.
Why Do Standard Sleep Remedies Make Histamine Intolerance Worse
Many standard sleep supplements do not address histamine clearance or mast cell mediator release. Melatonin interacts with mast cell pathways and may reduce some inflammatory signaling, but the available evidence does not show that melatonin alone resolves histamine-related insomnia. Fermented supplements and some probiotic formulations may also add histamine or histamine-producing organisms in sensitive individuals.
Melatonin is typically the first supplement people reach for when sleep is disrupted.