
Why Sleep Gets Easier to Break After Midlife
Scott Anderson interviewed me about what changes after 40, and why the same sleep advice stops matching the problem.

Today's piece is a little different: Scott Anderson interviewed me about sleep after midlife, why a full night can still leave someone unrested, what sleep trackers can show, and why 3 a.m. wakeups often need a more personal read.
Scott Anderson is a scientist and science writer who wrote the bestselling book The Psychobiotic Revolution (from National Geographic) with two of the top researchers of the gut-brain axis, John Cryan and Ted Dinan. He currently writes Psychobiotic: The Gut-Brain Revolution on Substack.
Below is our Q&A.
1. Is improving sleep different for men and women after midlife?
Yes, but not because men and women need totally different sleep.
The basics are still the same: enough sleep, steady timing, deep sleep, REM sleep, and fewer wake-ups.
What changes after midlife is the weak link.
In women, menopause can bring hot flashes, temperature swings, and waking up wired starting in the late 30's.
In men, I would look more closely at belly fat, testosterone function, waking to pee and breathing.
So the question is not only, "Did you sleep 7 hours?"
The useful move is to find your weak link first, because it is different for different people, often different for men and women, that is where sleep can improve again.
2. A lot of people sleep 7 or 8 hours and still wake up feeling unrested. What is usually missing from the "hours slept" conversation?
Hours are only time.
They do not tell us how well the sleep was built.
Good sleep also needs the right sleep stages, fewer breaks, and a rested morning.
Sleep stages means the brain moves through deep sleep and REM sleep in a normal pattern.
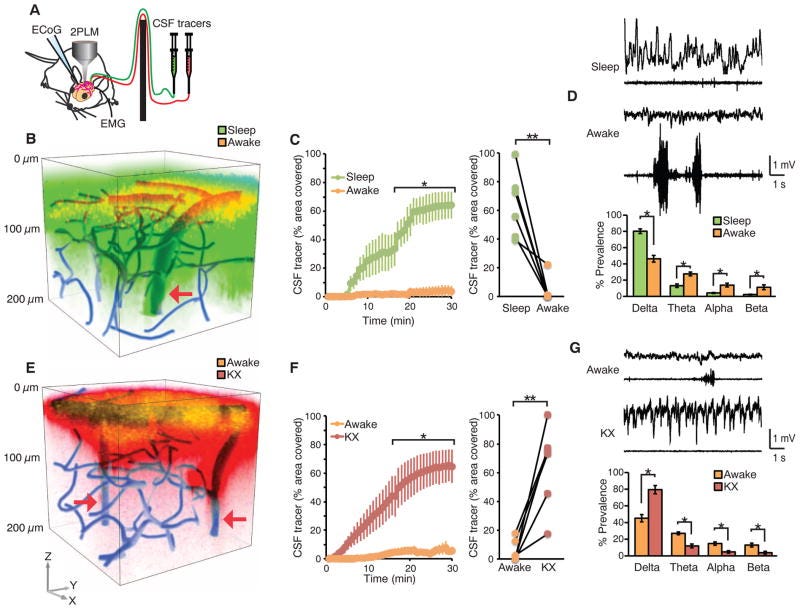
Deep sleep is the heavy sleep that helps repair the body and clear waste from the brain.
REM sleep is the dream stage that helps mood, memory, and emotional balance.
So a person can get 8 hours and still not get restful sleep.
The underappreciated strategy is actually to track restful sleep above everythign else, because quality, continuity, and morning restoration are the signs that tell us whether sleep is actually doing its job.
3. What does a sleep tracker still not tell us, even when it gives sleep stages, HRV, recovery scores, and total sleep time?
A tracker can show clues.
It can show short sleep, high heart rate, low HRV, or a rough stage estimate.
HRV means how much the heart rhythm changes from beat to beat.
But a tracker usually cannot tell you why the night went wrong.
It does not know if the 3 a.m. wake-up came from stress hormones, blood sugar, hormones, or body clock timing.
It also does not know why you woke wired, woke groggy, woke to pee, or could not fall back asleep.
The missing layer is translation: what pattern is this, and what should I test next?
This is where digging into your actual sleep patterns is useful: for example, what the wake-up felt like, when it happened, whether you woke wired, groggy, hungry, hot, or needing to pee, and what changed that day.
Then sleep advice becomes personal to the real pattern, instead of one more generic score.
4. How does sleep predict neurodegeneration? There is a strong link between poor sleep and Alzheimer's, but is poor sleep a cause or an early symptom?
This is a real chicken-and-egg question.
Both sides seem true.
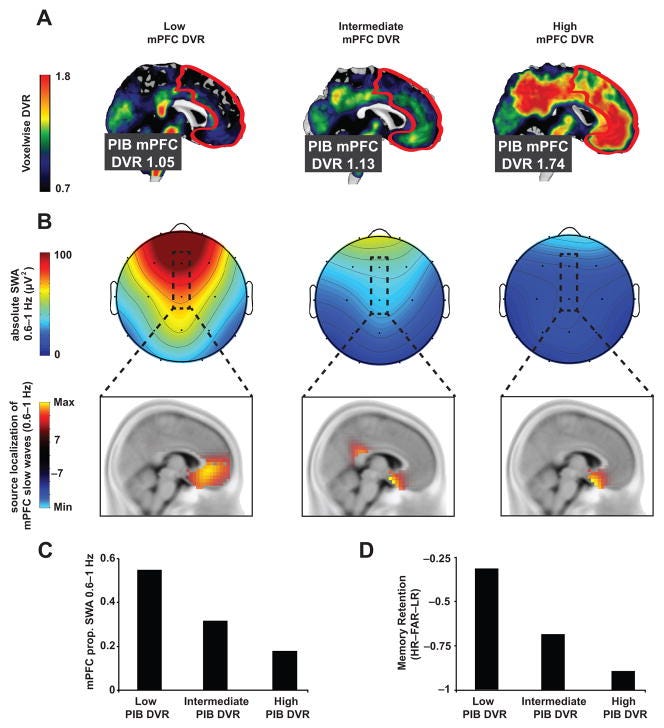
Bad sleep can raise Alzheimer-linked proteins like amyloid and tau.
Amyloid and tau are sticky proteins that build up in Alzheimer's disease.
But early brain disease can also damage the brain areas that control sleep.
In a Framingham study published in 2023 (incl Harvard researchers), each 1% annual decrease in deep sleep was linked with 27% higher dementia risk over 17 years.
So poor sleep can be both a risk signal and part of what speeds brain aging.
That makes sleep worth improving now, because steadier, more restorative sleep is one of the daily ways we support a younger brain.
5. Studies show a large increase in REM sleep for runners. Given the link between REM sleep, waste clearance in the brain, and Alzheimer's pathology, should we prioritize REM-boosting movements over deep-sleep-boosting ones as we age?
I would not make this a REM versus deep sleep choice.
Both matter.
The goal is natural sleep architecture, which means the normal order of light sleep, deep sleep, and REM sleep across the night.
Deep sleep seems especially tied to brain cleaning, including amyloid-beta, one protein linked with Alzheimer's disease.
REM sleep seems especially tied to mood, memory, and emotional processing.
Movement is useful because it can help the whole sleep system, not because we should chase one stage like a supplement.
So, the practical goal is steady training that helps you sleep deeper, dream normally, and wake restored.
6. Why do some people need less sleep? "Short sleepers" can function well with less than six hours of sleep without negative health effects. What are they doing differently?
True natural short sleepers are rare.
They are not just busy people who trained themselves to sleep less.
Many seem to have gene changes that alter sleep need.
Genes are instruction codes in the body.
Their brain may build enough recovery in less time.
For most people, feeling "fine" on 5 or 6 hours is not the same thing. Stress hormones can hide tiredness, so most short sleep is adaptation, not a superpower.
A better place to start is to gradually add sleep and see whether mood, stamina, focus, and morning energy improve.
7. Why can someone in their late 40s or 50s do all the sleep hygiene and still wake at 3 or 4 a.m.?
Because sleep hygiene only fixes sleep problems caused by poor sleep habits.
A dark room helps if light is the issue.
It will not fix address cortisol, inflammation, hormone function changes or metabolic contributors.
In midlife, the same small trigger can cause a bigger wake-up response.
That is why someone can fall asleep fine, then wake at 3 or 4 a.m. with a busy brain.
The better question is not, "What supplement did they miss?" It is, "What changed in the body that made sleep easier to break?"
That gives people a better starting point than another sleep hygiene strategy.
-Kat
P.S. If you're still waking up at 3am and waking up with a brain fog, I'm opening private early access to a science-backed sleep intelligence app for men 40+ focused on energy, clarity, brain health, and longevity, coming to iOS and Android.
Join the waitlist, or share this with someone you care about who could benefit.
References
Kruijver, F. P. M., & Swaab, D. F. (2002). Sex hormone receptors are present in the human suprachiasmatic nucleus. Neuroendocrinology, 75(5), 296-305.
Karatsoreos, I. N., Butler, M. P., LeSauter, J., & Silver, R. (2011). Androgens modulate structure and function of the suprachiasmatic nucleus brain clock. Endocrinology, 152(5), 1970-1978.
Windred, D. P., Burns, A. C., Lane, J. M., Saxena, R., Rutter, M. K., Cain, S. W., & Phillips, A. J. K. (2024). Sleep regularity is a stronger predictor of mortality risk than sleep duration: A prospective cohort study. Sleep, 47(1), zsad253.
Xie, L., Kang, H., Xu, Q., Chen, M. J., Liao, Y., Thiyagarajan, M., O'Donnell, J., Christensen, D. J., Nicholson, C., Iliff, J. J., Takano, T., Deane, R., & Nedergaard, M. (2013). Sleep drives metabolite clearance from the adult brain. Science, 342(6156), 373-377.
Mander, B. A., Marks, S. M., Vogel, J. W., Rao, V., Lu, B., Saletin, J. M., Ancoli-Israel, S., Jagust, W. J., & Walker, M. P. (2015). beta-amyloid disrupts human NREM slow waves and related hippocampus-dependent memory consolidation. Nature Neuroscience, 18(7), 1051-1057.
Kang, J. E., Lim, M. M., Bateman, R. J., Lee, J. J., Smyth, L. P., Cirrito, J. R., Fujiki, N., Nishino, S., & Holtzman, D. M. (2009). Amyloid-beta dynamics are regulated by orexin and the sleep-wake cycle. Science, 326(5955), 1005-1007.
Holth, J. K., Fritschi, S. K., Wang, C., Pedersen, N. P., Cirrito, J. R., Mahan, T. E., Finn, M. B., Manis, M., Geerling, J. C., Fuller, P. M., Lucey, B. P., & Holtzman, D. M. (2019). The sleep-wake cycle regulates brain interstitial fluid tau in mice and CSF tau in humans. Science, 363(6429), 880-884.
Ju, Y. E. S., Ooms, S. J., Sutphen, C., Macauley, S. L., Zangrilli, M. A., Jerome, G., Fagan, A. M., Mignot, E., Zempel, J. M., Claassen, J. A. H. R., & Holtzman, D. M. (2017). Slow wave sleep disruption increases cerebrospinal fluid amyloid-beta levels. Brain, 140(8), 2104-2111.
Himali, J. J., Baril, A.-A., Cavuoto, M. G., Yiallourou, S., Wiedner, C. D., Himali, D., DeCarli, C., Redline, S., Beiser, A. S., Seshadri, S., & Pase, M. P. (2023). Association between slow-wave sleep loss and incident dementia. JAMA Neurology, 80(12), 1326-1333.
He, Y., Jones, C. R., Fujiki, N., Xu, Y., Guo, B., Holder, J. L., Jr., Rossner, M. J., Nishino, S., & Fu, Y.-H. (2009). The transcriptional repressor DEC2 regulates sleep length in mammals. Science, 325(5942), 866-870.
Shi, G., Xing, L., Wu, D., Bhattacharyya, B. J., Jones, C. R., McMahon, T., Chong, S. Y. C., Chen, J. A., Coppola, G., Geschwind, D., Krystal, A., Ptacek, L. J., & Fu, Y.-H. (2019). A rare mutation of beta1-adrenergic receptor affects sleep/wake behaviors. Neuron, 103(6), 1044-1055.e7.
Xing, L., Shi, G., Mostovoy, Y., Gentry, N. W., Fan, Z., McMahon, T. B., Kwok, P.-Y., Jones, C. R., Ptacek, L. J., & Fu, Y.-H. (2019). Mutant neuropeptide S receptor reduces sleep duration with preserved memory consolidation. Science Translational Medicine, 11(514), eaax2014.